Posterior Lumbar Fusion
Here’s what you need to know about posterior lumbar fusion surgery:
Description of surgery
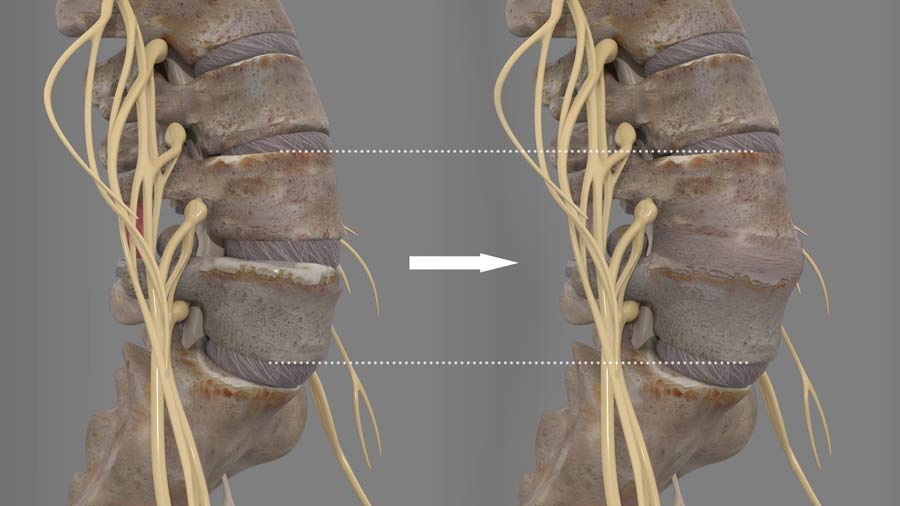
The purpose of the surgery is to fuse two or more vertebral bones of your lower back to one. This is achieved by tricking your body into thinking the individual vertebral bones are broken at which point your body attempts to heal this break into one bone.
The procedure begins with the surgeon making an incision along the midline of the patient’s back. The back muscles are gently moved to the side so the spine is visible. Usually, a fusion is performed together with the laminectomy procedure. As explained in a prior video, laminectomy removes boney pressure on the nerve sac. Fusion can be necessary after removal of stabilizing bone anatomy to solve complaints related to fractures, herniations, infections, or tumors.
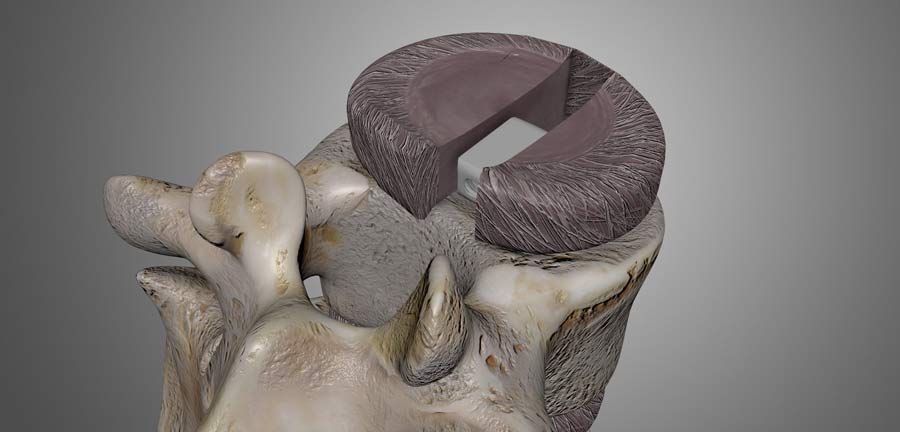
For the interbody fusion, the facet joint may be removed to expose and ensure the removal of the disc. The surgeon moves the spinal nerves to the side and replaces the disc with a bone graft or an interbody fusion device. Care is taken to protect the nerve sac during insertion of the interbody fusion cages. The additional space around the cage is then backed with bone material to support the healing process.
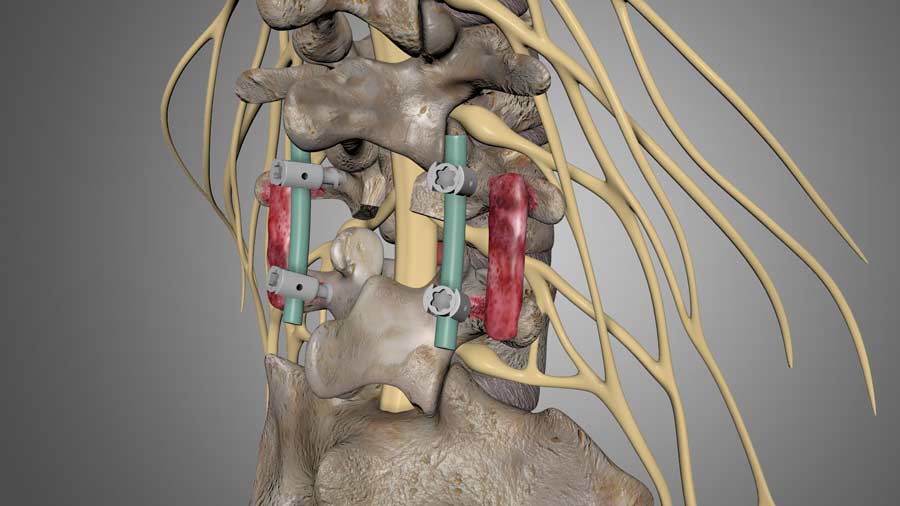
The spine must be stabilized for proper fusion to occur. A combination of screws and rods is used to achieve this stabilization of the spine. The screws can be placed in the pedicles, which are the strongest part of the spine. Rods and bolts are then used to fasten and link the screws to one another. Additional bone graft is placed along the sides of the vertebral bones.
PLF generally runs from two to five hours. Traditionally, patients were admitted to the hospital for a few days, but minimally invasive techniques now allow many to return home the same day of the surgery. Patients can expect to return to normal physical activities 3 to 6 months post-op.
Why get it?
Your doctor has considered this surgery if the examinations they conducted are consistent with your symptoms of pain. For bone spurs or disc findings: only after exhausting all non-surgical treatments should you consider this surgery. The primary candidates for PLF suffer from back pain caused by multiple recurrent disc herniations, spondylolisthesis, spinal fractures, or scoliosis. In rare instances, it can be necessary because of infection or tumors.
Why not? Complications
All surgeries have risks and potential complications. The most severe complications are neurological deficits and infection. Complications rates vary and depend on a variety of factors: the selected technique, the quality of the bone graft, the preoperative condition of the patient — to name a few. If you have any specific questions or concerns, please discuss them with your doctor.
Fusion Variations
There are many variations to PLF. Some Surgeons may utilize a pair of smaller incisions to minimize the invasiveness of the procedure. Others may place the interbody cage in an oblique direction. Some may even use the classic fusion technique of roughening the bones, placing bone graft, and using only a brace without any plates rods, or screw. Again, all of these options are considered with the patient’s best outcome in mind.
I hoped this helped your understanding of posterior lumbar fusion surgery. Until next time, this is Dr. John Shim.
Additional Resources:
https://doi.org/10.1016/j.jtumed.2013.01.007
Citations
- Okuda S, Miyauchi A, Oda T, Haku T, Yamamoto T, Iwasaki M. Surgical complications of posterior lumbar interbody fusion with total facetectomy in 251 patients. J Neurosurg Spine. 2006 Apr;4(4):304-9. PubMed PMID: 16619677
- Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015 Dec;1(1):2-18. PubMed PMID: 27683674
Last modified: March 10, 2021